So let’s say you’re having a bad day: you have bad enough abdominal pain that you decide it’s time to go to the ER.
Unfortunately, it’s not The Pitt: it’s my ER! Sucks to be you.
Bad fluorescent lights and plasticky chairs, a waiting room at capacity filled with vomiting children, and a wait that feels longer than you were prepared for. You get triaged and your vitals are taken. If you’re lucky, you wait three hours. You’re brought back to a room. A nurse asks you a bunch of dumb questions about whether you have guns in the home and whether you’ve recently traveled to Zambia. And then, someone walks in to see you.
Here’s the question: who is that person?
In your very near future, the answer is NOT going to be ‘a physician.’ Why?
First: Many emergency departments are staffed indirectly through a staffing company that often holds contracts at multiple hospital EDs. These companies are called contract management groups, or CMGs. If you work in an office building, chances are the housekeeping staff aren’t directly employed by your company – they’re employed by a CMG that your business contracts with.
Less commonly, ED docs are employees of the hospital, like me, or partners in a staffing company that only contracts with their home hospital called a small democratic group. These are vanishing across the country because CMGs offer an economy of scale and are often debt leveraged by private equity to mask their losses further – making them super appealing, financially, to a hospital system.
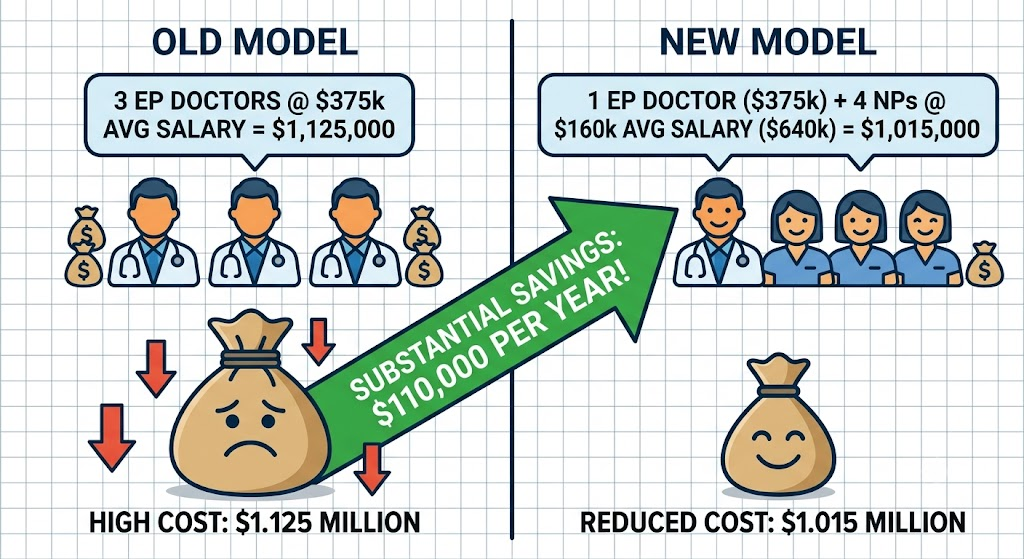
Second: An emergency physician costs, on average, somewhere in the neighborhood of $300-450k a year in total compensation, plus benefits. A nurse practitioner (or less commonly, a physician assistant) with independent practice authority – meaning they don’t legally need a physician to supervise them and carry their own malpractice insurance – costs somewhere between $120-200k. If you’re a CMG running many ERs, your entire success financially depends on extracting maximum margin from each site. This math is not subtle. Replace three ER doctors with one ER doctor and four NPs, and you have just saved a huge amount of money while maintaining the coverage you had before.
ChatGPT provides:
This is, to be clear, already happening. Currently somewhere between 20-40% of emergency department patients nationally are seen primarily by a nurse practitioner or physician assistant. That number is going to rocket upwards, not because it’s necessarily the right thing to do for patient care, but because the economics are overwhelming… and in over half of US states, NPs now have full independent practice authority. This means not only is NP usage growing, but the practitioners are not legally required to have supervision by a duly board-certified physician. The financial incentives are all pointing the same way – more NPs/PAs and less MD/DOs.
So here’s what the ED of the future looks like, operationally. There is one ER attending physician at a time, no matter how big your department.
(Okay, maybe two on busy shifts in bigger departments like mine).
The attending is not there to crank through 30 patients in 8 hours – they’re supervising a gaggle of NPs, mayyybe primarily handling the highest-acuity stuff (the actual crashing patients) and signing off on charts if the state doesn’t have full practice authority yet for the midlevels. The NPs are doing literally everything else that makes up 98% of the ED:
- rashes
- fevers
- abdominal pain
- heart attack and stroke workups
- back pain for six years
- things that are actually primary care/urgent care issues but no one can see their regular doctor for 5 months, or they lost insurance, or whatever.
And more. There are a million reasons why people come to the ED. 999,992 of them will be treated by an NP.
Does this model work?
Financially yes. From a quality of care perspective, no not really. An experienced emergency medicine NP who has been doing this for ten years is genuinely quite good at what they do. They have pattern recognition. They know when something feels wrong and can escalate to the attending. I’ve worked with NPs who I think are good enough to handle most ER cases. We have an NP that sees our ‘fast track’ patients – bumps, cuts, gastro, flu – and I largely trust her judgment.
(We also have a new NP who I do not trust to keep his fingers attached when chopping vegetables.)
If you staff your department with experienced NPs, the model functions pretty well, and the attending is freed up to focus on the people who need them most.
…BUT of course that’s not what’s actually going to happen. That would require a decades-long investment in high-quality NP training and clinical exposure, which requires foresight, which no one in healthcare policy is allowed to have. We are currently in the business of churning out a huge number of fresh new NPs who have practically zero clinical experience. Nurses are fleeing the bedside for the NP credential because it pays better and bedside nursing is destroying souls. Diploma mill programs with low bars to entry are cropping up left and right.
A new-grad NP seeing patients independently in an emergency department is… a choice! Not because NPs are bad clinicians (I mean, without real experience, yes they are), but because seeing sick undifferentiated patients in an emergency department is genuinely hard, the learning curve is steep and the consequences of being wrong are occasionally catastrophic. This is why we put physicians through four years of medical school and three or four years of brutal residency before we let them do it unsupervised. It’s not so much about gatekeeping or protecting physician turf – it’s about the fact that working in the ED is “walking through a minefield in clown shoes” as one of our aphorisms says.

But the new-grad NP is cheaper. So.
Meanwhile, the attending physician who is nominally “supervising” this pod of NPs is in a structurally bizarre position. They will have nominal supervisory responsibilities, but liability will be murky depending on the state. In theory, they should be available for complicated cases and to resuscitate the sickest of the sick; in most cases, they’ll be answering questions from the new-grad NP in room four every six minutes.
(I have tried to think of another profession that operates this way. A pilot supervising four student pilots each flying their own plane, maybe? The anesthesiology model is similar – one anesthesiologist can supervise a number of CRNA’s doing cases – but CRNA training is vastly deeper and more standardized than NP training.)
Ok so what. What does all this mean for me? What does this mean for us physicians, and the residency programs cranking out 2,500 new ER docs every year?
IT IS VERY BAD. (you didn’t think you’d make it through this without the usual pessimism, did you??)
If the dominant model of ED staffing shifts to one attending plus an army of midlevels, we simply don’t need 2,500 new ER doctors per year. I don’t know exactly how much we DO need, but it’s a lot lower. Something like a 30-50% decrease feels about right. With that kind of drawdown, residency programs will close.
Programs are not going to be cool about it, either: hospitals with trainees make crazy money off them! Did you know that a hospital training residents gets a huge chunk of money from Medicare per resident? And that the resident salary and administration costs are way lower than the value of the subsidy?
Also, residents are indentured servants, and servants are cheap. Hospitals won’t happily give up that free money and free labor!
Anyway.
What will happen first is the EM job market will tighten. New grads will have to take whatever jobs exist, usually at progressively lower pay as supply exceeds demand – this is already a major problem in desirable areas like NYC, San Diego, etc. Right now an after-hours plumber in San Diego has about the same hourly rate as an new emergency physician. Not exaggerating.
The jobs that do exist will increasingly look like “supervising four NPs and maybe seeing the sick ones” rather than “practicing full-scope emergency medicine.” In rural areas, there might not be an ER doctor for hundreds of miles – and again, this is already a major problem.
Some people will be fine with that. (Actually I’d be fine with that, but the pay dropping along with it is kind of a dealbreaker.) Others will do a fellowship to escape, which is what I did.
Over a half-decade or so, the weaker residency programs – the ones without strong academic infrastructure, without prestigious training hospitals, without powerful faculty with enough clout to protect them – will quietly merge or close. You’ll go from 200+ accredited EM residency programs today (I think?) down to something like 110 or 120. It will be slow and messy and no one will call it what it is, which is a professional rerating of need driven by a healthcare economy that no longer needs that profession.
The programs that survive will be the ones attached to Level I trauma centers and large academic medical centers, where the case mix is a bit higher acuity and the infrastructure to emphasize supervision and deemphasize ‘moving the meat’ can actually work. This will probably be worse for patient care, but remember in the American healthcare system the patient is the product, not the customer. On a societal level we only care about patient care insofar as it affects the bottom line (or bad PR, which indirectly affects the bottom line). Hospitals will make a superutilitarian calculation: are worse outcomes – medical code for ‘more deaths,’ along with the lawsuits and local news hits that come with them – an acceptable risk to take to cut costs and improve throughput? I think they will bet yes.
Also, Admitting physicians and consulting physicians will HATE this, because they are going to get way more calls and admissions from under-experienced and poorly-trained midlevels who don’t understand how to formulate a consult question. Patients are going to hate it (they already do, I hear “I can’t get in to see a doctor” 15 times a shift). Everyone will hate it except for the companies running the healthcare system, who should see their costs shrink, their profit margin expand, and additional value delivered for shareholders. That’s what it’s all about, right?

Otis sends his regards. He is untroubled by healthcare economics and is mostly concerned with guilting his owner into an unearned treat.

Ha! Well done friend. I feel proud being somewhat responsible for fertilizing your cynical seedling into the mighty strangler fig (look it up) it has become. You are missed here.
You’re 100% right and I don’t see much changing unless the majority of patients consistently refuse to be seen by an NP. Also there needs to be a few expensive, high-profile lawsuits where the NP cost the hospitals big time. But idk if even that would do it
You are back! I’m glad you’re writing again!
Glad you’re back to writing. Hi Otis!